For decades, the “gold standard” for treating Androgenetic Alopecia (pattern hair loss) has been limited to just two options: Minoxidil to stimulate growth and Finasteride to block hormones.
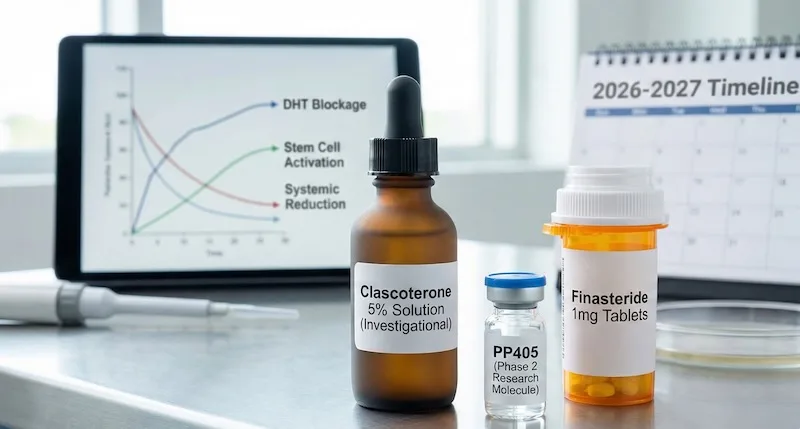
But the landscape is shifting rapidly. Following the release of pivotal Phase 3 data for Clascoterone 5% (late 2025) and promising Phase 2a results for PP405 (mid-2025), patients are looking at a future with more effective, safer choices.
At Derma Clinic, we believe in data over hype. This guide compares the two most anticipated future treatments—Clascoterone 5% and PP405—against the current market leaders to help you decide what is worth waiting for.
1. The “539% Improvement” Myth: Fact vs. Fiction
Recent viral headlines have claimed a “539% relative improvement” in hair growth for Clascoterone users. While this figure comes from legitimate Phase 3 trial data (SCALP 1), it is often misinterpreted.[1]
The Statistical Context
- Relative vs. Absolute Risk: The “539%” figure is a comparison against a placebo group. In hair loss trials, placebo groups often lose hair. If the placebo group loses hair and the drug group gains even a modest amount, the percentage difference mathematically skyrockets.
- The Clinical Reality: In absolute terms, Clascoterone 5% is a highly effective stabilizer. It stops hair thinning and promotes modest regrowth comparable to Topical Minoxidil. It is a major medical success, but it is not a “miracle cure” that will multiply your hair density by five times overnight.
2. Clascoterone 5% vs. PP405: The “Shield” vs. The “Wake-Up Call”
While Clascoterone is close to market, a newer competitor called PP405 (from Pelage Pharmaceuticals) is generating buzz with a completely different approach.
Clascoterone 5% (The Safe Shield)
- Mechanism: It is a Topical Androgen Receptor Inhibitor. It works by “shielding” your hair follicles from Dihydrotestosterone (DHT), the hormone that shrinks hair.
- Best For: Preventing further hair loss and maintaining what you have.
- Status: Phase 3 Complete (2025). Expected release: 2027.
PP405 (The Stem Cell Wake-Up Call)
- Mechanism: It is a Mitochondrial Pyruvate Carrier (MPC) Inhibitor. Instead of fighting hormones, it changes the metabolism of hair follicle stem cells. It forces them to switch from “resting mode” to “growth mode” (glycolysis) by increasing lactate production.[4]
- The Promise: It aims to “wake up” dormant follicles that have stopped producing hair, theoretically offering true regeneration rather than just maintenance.
- Status: Phase 2a Complete (2025). Phase 2b/3 starting 2026. Expected release: 2028–2029.
The Verdict: Which is Better?
- For Safety: Tie. Both are topical and have shown zero systemic side effects in trials so far.
- For Regrowth: PP405 shows higher potential for regenerating dormant hair, whereas Clascoterone is better at stopping the root cause of loss (DHT).
- The Future Protocol: They likely won’t be competitors. The ultimate treatment will be using Clascoterone to block the DHT damage and PP405 to force the follicles to grow—a “shield and grow” combination.
3. Clascoterone vs. The “Big 3”: Detailed Comparison
How does Clascoterone stack up against the medications you might already be using?
Clascoterone vs. Finasteride (Oral)
Oral Finasteride is the current king of preservation, reducing serum DHT by ~70%. However, because it works systemically (throughout the whole body), it carries rare but serious risks like loss of libido and erectile dysfunction. Why Clascoterone Wins: It offers a similar “anti-DHT” protection but does it locally on the scalp. Once it enters the bloodstream, it metabolizes into an inactive form, meaning it has zero sexual side effects. It is the “peace of mind” alternative to Finasteride.
Clascoterone vs. Minoxidil (Topical)
Minoxidil is a vasodilator—it widens blood vessels and forces hair into the growth phase. However, it does nothing to stop the hormonal attack (DHT) that is killing the follicle. Why Clascoterone Wins: Minoxidil is like watering a plant while someone is stepping on it. Clascoterone stops the “stepping” (DHT). While Minoxidil might grow hair faster in the short term, Clascoterone protects the hair long-term. The Pro Tip: Use them together. They work via completely different pathways and are safe to combine.
Clascoterone vs. Dutasteride
Dutasteride is the “nuclear option”—blocking over 90% of DHT. It is incredibly effective but carries higher risks of side effects than Finasteride. Why Clascoterone Wins: For patients with mild-to-moderate hair loss, Dutasteride is often overkill with unnecessary risk. Clascoterone offers a balanced approach: sufficient protection for the scalp without altering the body’s entire hormonal profile.
4. Timeline & Cost: What to Expect
- Release Date of Clascoterone 5%:
- Spring 2026: Completion of long-term safety data.
- Late 2026: FDA Filing.
- Mid-2027: Expected US Pharmacy Launch.
- Projected Cost: Based on the pricing of its acne counterpart (Winlevi), we estimate a retail price of $90 – $150 USD per month. Insurance coverage is unlikely for hair loss diagnoses.
5. Comprehensive Clascoterone 5% Analysis: Men vs. Women
Unlike Minoxidil, which works universally by stimulating blood flow, Clascoterone is a hormonal treatment. This means its efficacy varies significantly based on gender and age.
For Men: The Primary Candidate
The recent Phase 3 trials (SCALP 1 & SCALP 2) were conducted exclusively on males. The results were statistically significant across all endpoints.
- Ideal Patient: Men with early-to-moderate Male Pattern Baldness (Norwood Scale 2-4) who want to stop loss but are afraid of oral Finasteride side effects.
- Verdict: It will be an FDA-approved, first-line therapy for men.
For Women: A Complex Picture
The efficacy of Clascoterone in women is nuanced and depends heavily on age and hormonal status.[3]
- Women Under 30: Phase 2 trials indicated that younger women saw statistically significant improvement. In this age group, hair loss is often driven directly by high androgen sensitivity (similar to male pattern loss), making the drug highly effective.
- Post-Menopausal Women (Over 50): The drug showed reduced efficacy in older women compared to Minoxidil. In post-menopausal hair loss, the driving factors are more complex (lower estrogen, general aging) rather than just DHT, making an anti-androgen less effective as a standalone cure.
- The Safety Advantage: Despite mixed efficacy in older groups, Clascoterone fills a critical safety gap. Currently, women of childbearing age cannot take oral Finasteride or Dutasteride due to the risk of birth defects. Since Clascoterone is not systemic, it may become the safest off-label hormonal option for young women planning families.
6. Frequently Asked Questions (FAQ)
1. Is Clascoterone 5% a cure for baldness?
No, there is no permanent cure. It is a lifelong treatment. If you stop applying it, hair loss will resume within months.
2. Is PP405 better than Clascoterone?
They do different things. PP405 is better at waking up dormant hair (regenerative), while Clascoterone is better at protecting existing hair from hormones (preventative).
3. Will Clascoterone lower my testosterone or libido?
No. This is the main selling point. Clinical trials show no significant change in serum testosterone because the drug is metabolized before it affects the body systemically.
4. Why is the 5% concentration important?
The 1% concentration (Winlevi) is approved for acne but is too weak to penetrate the scalp effectively. The 5% formulation is essential for hair follicles.
5. Can I use Clascoterone with Minoxidil?
Yes. In fact, dermatologists expect this to be the standard non-pill regimen.
6. Will it work on a completely bald smooth scalp?
No. Like all current treatments, Clascoterone requires a living hair follicle. PP405 shows more promise for dormant follicles, but even that cannot revive dead (scarred) skin.
7. Is it better than RU58841?
Clascoterone is the only topical anti-androgen with Phase 3 safety data and FDA regulatory backing. RU58841 is an experimental research chemical with no human safety trials, making Clascoterone the much safer choice.
8. What are the side effects?
In trials, side effects were limited to local skin reactions: mild redness, scaling, or itching at the application site.
9. Will it be available for women immediately?
The initial FDA label will likely be for men. However, doctors can and likely will prescribe it “off-label” for female patients immediately after launch.
10. How often do I have to apply it?
The current trial protocol requires twice-daily application (morning and night).
11.Can I just buy the acne cream Clascoterone 1% (Winlevi) and use it on my head?
This is not recommended. The vehicle (cream) is designed for the face, not the scalp, and it contains only 1% active ingredient, which is likely insufficient to stop hair loss.
Final Verdict: Don’t Wait for 2027
Clascoterone and PP405 are game-changers, but waiting two years for their release is a mistake. Once a follicle dies, it cannot be revived.
Protect the hair you have now. Schedule a consultation with Derma Clinic Kathmandu (Call 9801358600 / Whatsapp / Direct Online Appointment) to design a scientifically proven treatment plan using currently available, FDA-approved options while we await the future of hair restoration.
References & Footnotes
- Cosmo Pharmaceuticals N.V. “Cosmo Announces Breakthrough Phase III Topline Results from SCALP 1 and SCALP 2 for Clascoterone 5% Solution.” Press Release, Dec 3, 2025.
- Rosette C, et al. “Cortexolone 17α-Propionate (Clascoterone) is an Androgen Receptor Antagonist.” Journal of Drugs in Dermatology, 2019.
- Pelage Pharmaceuticals. “Pelage Pharmaceuticals Announces Positive Phase 2a Clinical Trial Results for PP405.” Press Release, June 17, 2025.
- Flores A, et al. “Lactate dehydrogenase activity drives hair follicle stem cell activation.” Nature Cell Biology, 2017. (Scientific basis for PP405 mechanism).
Medical Disclaimer: The content provided in this article is for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.